The judging panel commended the reporting team for shining a light on “compounding tragedies and unfairnesses,” and putting together a “riveting package” of “love and loss in the face of adversity.” They praised Joe Mozingo for the “depth” of his reporting, and for “refusing to describe his subjects as ‘victims,’” instead portraying them “as warriors who are fighting hard battles, whether it's against the ravages of COVID-19 or structural racism.” They hailed the “compassion, care and visual power” of Francine Orr’s photography, saying it’s “clear how hard the reporting duo worked to gain the trust of the hospitals and their sources,” depicting “heroes of stories that are about survival.” Originally published by The Los Angeles Times between February and December, 2021.
By Joe Mozingo | Photography by Francine Orr | Los Angeles Times | February 19, 2021
Gilbert Torres sat in his hospital bed, sheets wrapped around his legs, clutching his phone with trembling hands.
Three weeks before, he was working his shift at a truck wash on South Alameda Street, counting the minutes before he’d be home playing with his 5-year-old boy.
Now such moments were just a beautiful dream.
In the hallway, nurses peered through the glass doors, wiping their eyes as they watched him confront the possibility that he might have minutes left to live. He was only 30 years old. He looked desperately alone.
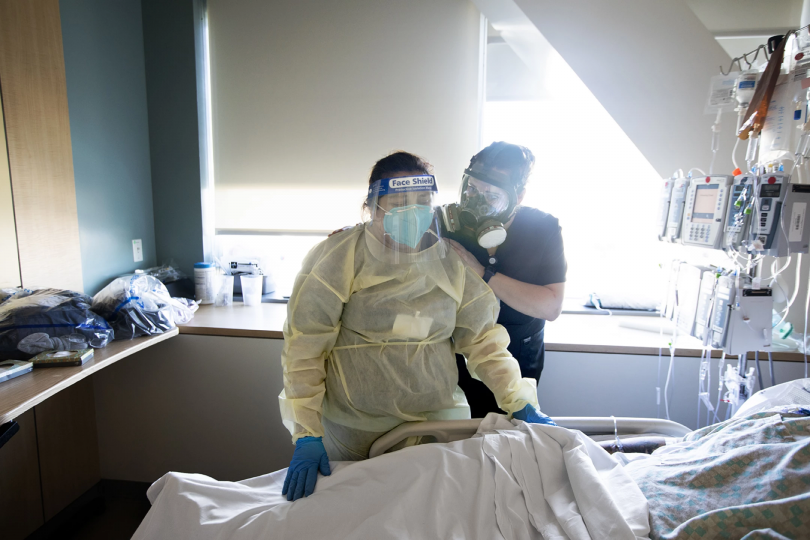
Nurses in white Tyvek suits and respirators stepped into the room to set up the ventilator.
Torres said goodbye to his girlfriend of nine years on video chat, laboring to get the words out. Even on high-flow oxygen through his nostrils, he struggled to breathe. He hadn’t slept in days.
He watched a team of nurses and doctors suit up in the hall.
Francine Orr / Los Angeles Times
Gilbert Torres, 30, in a better moment, sits up next to his bed at Martin Luther King Jr. Community Hospital.
An emergency room doctor leaned in and told him it was time.
Torres turned off the phone.
Francine Orr / Los Angeles Times
Dr. Jason Prasso checks on Gilbert Torres in the ICU at Martin Luther King Jr. Community Hospital on Jan. 20, the day after he was intubated.
The team came in. Wearing a bulky hood over his respirator and mask, the doctor stood behind him with the laryngoscope, ready to insert the breathing tube. A nurse released sedative and paralytic medications into Torres’ bloodstream.
He closed his eyes, clasping her hand.
:
They call it el tubo, and it haunts places like South Los Angeles, the Latino-majority neighborhoods hit harder by COVID-19 than almost anywhere in the U.S.
Intubation has become more than a medical procedure. It represents the terrible crossroad of this disease: the moment patients must decide whether to have a tube inserted into their trachea so a machine can take over their breathing.
While the procedure itself is relatively simple, it can spin out of control within seconds. The airway team generally puts the patients to sleep and stops their breathing. If their blood pressure isn’t stabilized as the rush of adrenaline abruptly falls off, or a doctor cannot secure the tube at the right spot quickly enough, oxygen levels drop precariously, leading to organ failure and death. But for people with severe COVID-19, the procedure can be the last bid for survival.
Arriving at this juncture presents one of the most agonizing choices a patient or family may ever have to make. Most people have no plan for what to do.
The only other option is to struggle on, with doctors managing the pain and anxiety with medication, as they lose oxygen and blood pressure and likely fall into cardiac arrest.
Most patients at this late stage will die whatever road they choose. While chances of survival might be higher on the ventilator, doctors say, those who recover could be left with major disabilities, including brain damage, severe respiratory problems and kidney failure. Younger people with no major underlying medical conditions fare better.
Francine Orr / Los Angeles Times
COVID-19 patient Mariano Zuñiga Anaya, 57, struggles to get enough oxygen at Martin Luther King Jr. Community Hospital.
With so many people going to hospitals for COVID-19, many South Los Angeles residents have stories about going on the tube: the uncle who died just minutes after hanging up with his family. The friend’s father who came out alive but would need dialysis the rest of his life. The aunt who died after three weeks in a coma. The middle-age cousin who is recovering.
At the heart of the suffering is Martin Luther King Jr. Community Hospital, a privately managed, high-tech facility that replaced the troubled county medical center that had closed in 2007. The Willowbrook hospital has been packed with patients facing the terrible choice.
Mariano Zuñiga Anaya, 57, knew all about el tubo. His older brother died in May on a ventilator in Mexico.
Now Zuñiga was sick in the small apartment in Florence-Firestone that he shared with his daughter Ana and her 5-year-old girl and 2-year-old boy.
Francine Orr / Los Angeles Times
Mariano Zuñiga Anaya in the ICU at Martin Luther King Jr. Community Hospital.
Zuñiga was a traditional show-no-weakness father who had turned into a playful, doting grandfather. He let his granddaughter paint his toenails and grandson draw “tattoos” all over his body with markers. He helped her learn how to read and write, and loved to listen to the stories she imagined up. They loved their abuelito.
Ana Zuñiga Diaz, 30, relished this new side of her father, and she was terrified now. Her mother and older sister still lived in Michoacán, and all the weight of his illness fell on her.
On Jan. 22, her dad was too weak to get up, could not eat and had a frantic, ragged cough. He had major health problems already, weighing over 275 pounds, with diabetes, hypertension and high cholesterol. He recently had lost part of a toe due to complications of diabetes.
Francine Orr / Los Angeles Times
Mariano Zuñiga Anaya lies prone to help increase his oxygen level.
Ana called her sister, Leslie, to explain his bad condition.
“She’s exaggerating!” her dad called out.
The family in Mexico feared if he went to a hospital he would be forced on a ventilator. Their uncle was dead within four days of getting intubated. They could not bear losing him the same way.
Back home in the mountain town of Zacapu, Mariano was a booming, fun-loving presence — the worker who left as a teenager, diligently sending money back for nearly 40 years. Twice a year he would return, hosting big fiestas with mariachi bands. He had a deep laugh and loved to joke and tell stories. Ana suspects he got COVID-19 on his flight back to Los Angeles after the New Year.
The family wanted him to stay out of the hospital, fearing it would be his death.
As Ana spoke to her sister, Mariano started coughing so violently it sounded like he was drowning. She hung up and called 911. The paramedics came and told him he had to go to the hospital. His blood-oxygen level was dangerously low. She felt helpless as they loaded him onto a gurney and took him away.
Francine Orr / Los Angeles Times
As a doctor performs an intubation on Gilbert Torres, a team of nurses and specialists wait outside in case complications arise.
Torres, the young father, lay on his belly, unconscious on the fifth-floor ICU three days after his intubation. His ventilator pumped with its eerie hiss-tap-tap metronome. Nurses talked gently to him as they repositioned him or checked his settings.
Dr. Joseph Meltzer, a UCLA critical care specialist working at the community hospital during the surge, had told Torres that he had to be intubated. But he made a promise: “We can get you through this.”
Now, Torres was stable, but his oxygen saturation fell every time he was turned to lie on his back, which he needed to do for eight hours a day to avoid blood pooling. Meltzer turned up the pressure on the ventilator to bring his oxygen up. But too much pressure, over too much time, could damage the tiny sacs in the lungs where oxygen was absorbed into the blood and carbon dioxide released, reducing his odds of surviving.
Francine Orr / Los Angeles Times
A doctor and nurse comfort Mariano Zuñiga Anaya as he struggles to keep his oxygen levels up before intubation
The same morning, Zuñiga was wheeled to the south wing of the telemetry unit on the first floor, room 710 — four doors from the room where Torres was intubated. Since the surge, the unit was filled to capacity, and became the transition zone where COVID-19 patients recovered enough to go home, or went to the ICU on a ventilator.
Zuñiga was in bad shape. Doctors put him on high-flow oxygen through his nose. They set the machine to 60 liters per minute. Only the ventilator could deliver more.
He lay on his side and his shortness of breath gradually abated, but his blood-oxygen level remained perilously low. He was at risk of organ failure. Talking or moving made it worse.
Francine Orr / Los Angeles Times
Nurse Jess Esperti holds Mariano Zuñiga Anaya’s hand to relieve his anxiety about intubation.
His granddaughter Hayley sent him little audio texts. “You’re going to be alright grandpa,” she said. “Echele ganas.” Give it your best.
Ana called him every morning.
“How are you feeling, Papa?”
“Estoy bien,” he would say in a robust voice. I’m good.
Francine Orr / Los Angeles Times
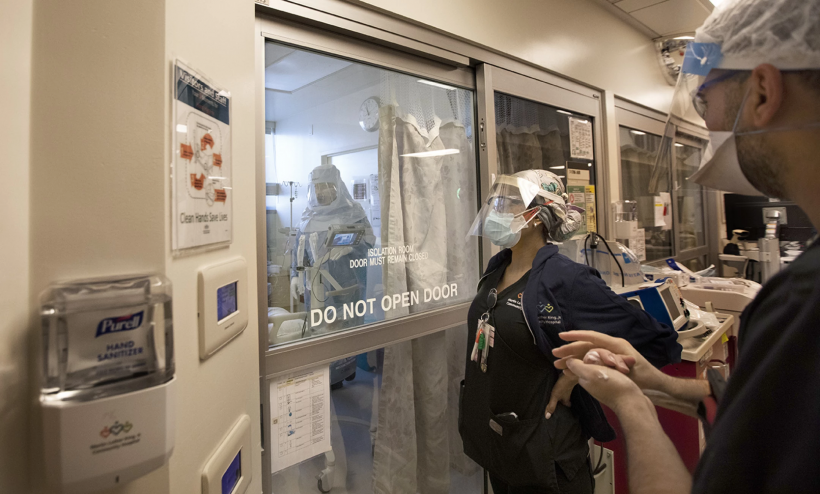
Nurse Fernando Fernandez pokes his head through the plastic covering a doorway in the ICU of Martin Luther King Jr. Community Hospital.
ADVERTISEMEN
But the doctors told her he was at a critical point. His oxygen delivery was at the maximum setting, and his blood saturation was not improving. They brought up the possibility of putting him on the ventilator, but he had refused it. When a reporter asked him why one day, he declared: “For fear, nothing else.”
The next day, Torres appeared to be rounding the bend. His blood pressure and oxygen levels were stable enough to gradually lower the pressure on the ventilator, to let his own breathing slowly take over.
On Jan. 24, Dr. Jason Prasso, a pulmonary and critical care specialist, decided Torres was ready to get off the ventilator. His team eased off the sedation.
But as Torres came to a low level of consciousness — still deeply blurred by the fentanyl — he grew agitated. They gave him an anti-anxiety medication as the respiratory therapist began to pull out nine inches of tube from his trachea.
When it came out, Torres panicked, struggling for air.
“Please intubate me,” he said. “I beg you!”
He grabbed Prasso’s hand.
Francine Orr / Los Angeles Times
Nurse Michelle Goldson cleans her face shield after exiting a patient’s room. Negative pressure in the room keeps the contaminated air from flowing into the hallways.
“Just relax, breathe,” the doctor said. “I can’t put it back in you. You’ve made it through so much.”
“Imagine you’re on a beach in Hawaii,” someone said.
“Please!” said Torres. “Knock me out, put me under.”
When the anti-anxiety meds kicked in, Torres floated around in a fog. Why was he in Hawaii? He didn’t have his glasses, so he couldn’t see anything but muddled colors, blue sky in the day, circles of light in the dark night. The sounds were so jarring and constant, so alien: the beeping of the monitors, the hiss of his roommate’s ventilator, muffled voices through the door.
Every so often the loudspeaker blared “Code Blue.” “Oh my God somebody is dying,” he thought. He started to cry.
In a couple of days, his mind started to sort itself out. But he had no memory of his days before the intubation or how he got to the hospital. In his haze, he tried to figure out why he was taken to one in Hawaii.
Francine Orr / Los Angeles Times
Nurse Jess Esperti adjusts the mask on COVID-19 patient Mariano Zuñiga Anaya. Every time he removes the mask to talk to his daughter, his oxygen levels drop.
Zuñiga continued to struggle after four days on maximum oxygen.
Dr. Krupa Gandhi noticed that “DNI” — do not intubate — was written in his notes. Seeing that he was only 57, she wanted to make sure that he understood what this meant.
She stepped into the room with a live translator on an iPad stand to speak with him in Spanish. Gandhi explained that if his vitals started to drop, the only way to save him might be the ventilator.
“I don’t want to be intubated. I want to die in peace,” he said. “I don’t even understand why you’re asking me this.”
He seemed to think he was doing well.
“You’re on a high oxygen requirement, and if you need more, you’re going to do worse,” she explained. “We have to know what your wishes are, so we have this conversation early.”
Zuñiga was adamant about not being intubated.
Even though he neared a point of no return, Zuñiga looked relatively relaxed. He wasn’t gasping for air, breathing rapidly, shaking or sweating. Every time a Times reporter visited him to see how he was doing, he always announced, in his strong voice: “Bien.”
“I think he just felt so comfortable that he’s like, no, I don’t need a tube,” Gandhi recalled shortly after her conversation. “I don’t know if his decision will change if he starts becoming more uncomfortable.”
Upstairs, Torres was moved back to telemetry, transitioning through the unit in the right direction this time. He could sit in a chair and look out the window. He had gone down the oxygen requirement chain to a simple cannula delivering a low flow of oxygen through his nose.
He was deeply shaken. He talked to his girlfriend, Lisseth, on the phone but couldn’t bring himself to talk to his 5-year-old son, Austin. Just thinking about it brought him close to sobbing. He missed him so much, and he didn’t want his boy to see him cry.
He was racked with anxiety over the trauma of the last week.
“It was the most scariest experience you could possibly have. You know why?” he recalled in a shaky voice. “Because you’re alone. Because you’re alone. That’s it. You’re alone.”
On Feb. 1, three days after Zuñiga rejected any option to be intubated, Dr. Ameer Moussa noticed that his oxygen and blood pressure were dropping. This would be the point to intubate before his organs failed.
“How are you feeling?” Moussa asked.
“Bien,” Zuñiga said.
“Any pain?”
“None.”
Moussa told him his condition was getting worse, that he could go into cardiac arrest at any moment, and asked him again if he wanted to be put on the ventilator.
“No,” Zuñiga said.
“Are you sure?” the doctor asked.
Zuñiga wavered. “Ask my daughter.”
Francine Orr / Los Angeles Times
Ana Zuñiga Diaz was left to call family members in Mexico to decide whether her father should be placed on a ventilator. His brother died on a ventilator in May.
The call from Moussa spun Ana into despair. She did not want this decision on her shoulders. Over the next hours, she called her sister in Mexico, then a cousin who was a doctor, then her dad.
Every time her father talked to her, his oxygen plummeted.
“These calls are making him worse,” said the nurse watching the monitors.
Ana finally called Moussa with the consensus that if he went into cardiac arrest they should try to resuscitate him and put him on the ventilator then — but not before. The doctor sighed. That didn’t make sense.
Francine Orr / Los Angeles Times
The airway team, led by Dr. Stefan Richter, prepares to intubate Mariano Zuñiga Anaya so he can be put on a ventilator. The procedure is risky, but can be the only way to save the life of a patient with severe COVID-19.
He went back to Zuñiga with the iPad translator, trying to understand his thinking.
He asked him why he wanted to be intubated only if his heart and lungs stopped.
“Vivo,” he said. Alive.
“If you want to live, then the best thing is to intubate now and not when it’s too late,” Moussa said.
Zuñiga was silent. “Does it hurt? he asked.
“No, I put you to sleep.”
Zuñiga stared up at the ceiling, thinking it over.
“Esta bien.”
Within 20 minutes of Zuñiga’s decision, Dr. Stefan Richter arrived from the ICU to carry out a procedure he had done hundreds of times — but which could still go disastrously wrong.
COVID-19 patients have usually been under a flood of adrenaline for days. The moment the sedative hits the brain, that drops off and their blood pressure tends to crash.
A minute later, the paralytic hits, and the patients’ breathing stops. With COVID-19 patients who were already severely oxygen deprived, it leaves the doctors seconds to thread the tube through the larynx into the trachea. And that small gap, next to the opening of the esophagus, can be hard to find.
Richter said a fraction of patients die within minutes or a couple of hours after intubation.
A dozen nurses and specialists waited outside room 710, ready for any possible emergency. Two nurses and a respiratory therapist assisted the doctor in the room.
Francine Orr / Los Angeles Times
Mariano Zuñiga Anaya tears up slightly as he prepared to be intubated, knowing this could be his last moment of consciousness before death.
At the center of this swirl of activity, Zuñiga lay still, silent and scared, tears glistening in his eyes.
The ICU nurse released the short-acting sedative etomidate into his IV, followed by the paralytic rocuronium. Zuñiga fell asleep almost instantly, avoiding one of the very rare but terrifying moments a human can experience: having the paralytic hit while they are still awake.
Richter took the sickle-shaped video laryngoscope and ran it down the right side of Zuñiga’s tongue, pushing it to the side to clear a path to the larynx. A camera and light at the tip of the sickle guided the way, displaying the image on a small screen on top of the scope. Richter guided it through folds of excess tissue, looking for the opening.
Zuñiga’s oxygen monitor rang an alarm as his blood saturation dropped below 80%. The respiratory therapist silenced it.
“Pressure is dropping; why don’t we start Levo?” Richter asked the ICU nurse.
Francine Orr / Los Angeles Times
Mariano Zuñiga Anaya is put in an induced coma and paralyzed as Dr. Stefan Richter begins the intubation procedure.
Levophed supplemented his falling adrenaline, constricting his blood vessels to build the pressure back.
Richter spotted the opening, a small hole between the vocal cords, and ran the tube down a groove in the scope to guide it through. He stopped at 26 centimeters below Zuñiga’s front teeth. He pulled out the stiff wire that kept the tube from crimping and asked the respiratory therapist to inflate “the cuff” — a balloon around the tube that seals it to the trachea, keeping the pressure in the lungs.
A probe attached to the ventilator showed carbon dioxide coming out of the tube, a good sign it was in the right spot. Richter still wanted to be absolutely sure the tube hadn’t gone down the esophagus, which could be fatal if not fixed instantly. He took a stethoscope to Zuñiga’s stomach to listen for any airflow there. There was none. He listened to the lungs with his stethoscope and could hear air flow.
They all stared gravely at the iPhone-sized monitor on Zuñiga’s chest. His oxygen had crashed to 6%, a level that would rapidly kill him.
His blood pressure was down too, at 70/30, creating a potential shock to the kidneys and other organs.
The therapist let a burst of air from the ventilator to open any air sacs in the lungs that had collapsed during the procedure.
Slowly, Zuñiga’s numbers began to recover as the ventilator and vasoconstrictors did their work.
He was wheeled to the ICU with oxygen numbers in the low 90s and blood pressure of 100/70. But the initial crash in both loomed as a bad omen.
::
Francine Orr / Los Angeles Times
Gilbert Torres recovering after five days on a ventilator in the ICU. He recalled the first days he was taken off the ventilator as terrifying and disorienting.
On the bright, crisp morning of Feb. 6, Torres was ready to go home. He beamed in happy disbelief. He put on an Avengers T-shirt and packed up his items.
A doctor came in and listened to his lungs and advised him to be alert for any new symptoms. He was still weak and needed oxygen. He’d have to come back to the post-release clinic in a week for doctors to check his progress.
Torres was wheeled out the modern glass entrance of Martin Luther King Jr. Community Hospital, smiling like a little boy.
He wept as his girlfriend walked up to him. She gave him a long hug.
Francine Orr / Los Angeles Times
Gilbert Torres smiles as he waits to go home after more than three weeks at Martin Luther King Jr. Community Hospital.
The senses overwhelmed his emotions: her smell and touch, the sunlight and the cool breeze. “I missed you so much,” he said.
They loaded the wheelchair in the back of her sister’s car. He got in the backseat with his oxygen tank.
He knew he’d never be the same. Since he left the ICU, he promised God he would be a better man, someone his son would be proud of. He had made this vow over and over, and he had no doubt he would keep it.
“Can we just drive awhile?” he asked.
He opened the window and took as deep a breath as he could. He wanted to stay outside forever.
As they rolled along Central Avenue, he reached out the window and let his cupped fingers sail through the air, angling up and down, right and left, such a simple joy flying his hand in the wind.
::
At that very moment, Ana Zuñiga was on the fifth floor. Prasso had called her earlier that morning.
Two days after the intubation, Mariano Zuñiga’s kidneys shut down and he had to be put on continuous dialysis. Healthy kidneys use carbon dioxide to regulate blood acidity. His failing ones put a larger burden on the lungs to expel the gas.
Zuñiga’s acid level was rising while oxygen and blood pressure were dropping.
This was the end. Earlier that morning, Prasso stopped the dialysis and returned all his blood to his body to stabilize the pressure, just to give Ana enough time to come see him.
“There’s nothing else I can do for him,” Prasso said.
A nurse gave her a long hug.
Francine Orr / Los Angeles Times
Nurse Jesse Garcia comforts Ana Zuñiga Diaz before Ana says her final goodbye to her father.
Prasso explained that without dialysis her father was going to die within a day.
“Now if he could step out of his body right now, understand everything that was going on, how do you think he would want to pass?” he asked. “Would he want to pass attached to all these machines, or pass more naturally?”
“He wouldn’t want to die on all these machines,” she said without pause.
He had the nurses give her father medication to tamp down any pain, nausea and shortness of breath. At 11:05 a.m, they removed the tube. Zuñiga had no visible response. His mouth stayed open.
Ana put on a medical gown, face shield and N-95 mask and entered his room.
Francine Orr / Los Angeles Times
Ana Zuñiga Diaz says goodbye to her father, hugging him moments after he died. As his vitals were dropping, she stroked his cheek and tucked him in.
“Papa,” she said. She came to his side and gently closed his mouth. “I love you.”
She took deep breaths through her nose to keep from sobbing. She patted his arm and took care to tuck him better into his sheet.
“Wherever you are, I want you to be happy,” she said.
She clasped her father’s hand, hugged him and cried.
Francine Orr / Los Angeles Times
Nurse Christy Converse embraces Ana Zuñiga after her father died. “I feel so alone,” Ana said.
She didn’t know what she was going to tell her daughter. Hayley was so close to him, always sneaking in her abuelo’s room to check on him. His absence in their small apartment would be an inescapable hole.
Ana Zuñiga held him quietly and prayed.
“Please go in tranquility and peace. We are all going to be fine. We will always remember you.”
Joe Mozingo is a projects reporter for the Los Angeles Times. He won a Robert F. Kennedy Award for covering the earthquake in Haiti and the ASNE Punch Sulzberger Award for Online Storytelling for his in-depth look at a federal investigation into relic poaching in rural Utah that led to three suicides. Mozingo helped lead The Times’ coverage of the Isla Vista killings in 2014 and a Miami Herald investigation into the space shuttle Columbia crash in 2003; both were finalists for the Pulitzer Prize. His book, “The Fiddler on Pantico Run: An African Warrior, His White Descendants, a Search for Family” was a 2012 “Discover Great New Writers” pick by Barnes and Noble.
Francine Orr
Staff Photographer - Los Angeles Times
Francine Orr has been a staff photographer for the Los Angeles Times since 2000. Previously, she was as a staff photographer at the Kansas City Star. Orr served as a Peace Corps Volunteer in Yap, Federated States of Micronesia. While there, she learned how to be a quiet observer and gained a love for stories. She was raised in Colorado and earned bachelor’s degrees in both history and art from the University of Saint Mary. Orr has focused on public health and poverty issues in Africa, India and the United States. In Los Angeles, she has concentrated on the growing homeless crisis since 2005. Orr received the coveted 2020 Meyer “Mike” Berger for an outstanding example of in-depth, human interest reporting from Columbia Journalism School. She was a Pulitzer Prize finalist in feature photography in 2012. Other awards include the Casey Medal for Meritorious Journalism, honors from Investigative Reporters and Editors, the Center for Public Integrity’s Daniel Pearl Award, Pictures of the Year International, National Press Photographers Assn., Society of Newspaper Design, Sigma Delta Chi Award for Public Service, Harry Chapin Award, Los Angeles Press Club, National Headliner Award, Sidney Hillman Award and Press Photographers of Greater Los Angeles.
Hector Becerra
Deputy Managing Editor - Los Angeles Times
Hector Becerra is the deputy managing editor for California and Metro, at the helm of our largest staff with a charge of refining its mission and mining for new coverage gold. He oversees the coalition of beats, teams and distinctive voices that comprise our signature local and statewide coverage — from the 88 cities in greater L.A., to our evolving approach to communities of color, investigative journalism and the narratives that define the contours of the most populous state in America.
Robert St. John
Senior Photo Editor - Los Angeles Times
Robert St. John is a senior photo editor at the Los Angeles Times. He joined the newsroom in 1998 from the Detroit Free Press, where he was deputy director of photography.
Request Publications
Tragedies & Journalists
A 40-page guide to help journalists, photojournalists and editors report on violence while protecting both victims and themselves.
This documentary, available online and on DVD, features a wide range of Australian journalists their recounting experiences covering traumatic stories.
Whether clinicians like it or not, children and families affected by trauma are routinely covered by the media. When that happens, clinicians often face difficult choices.
In conjunction with the Australian Broadcasting Corporation, Dart Centre Asia Pacific created a teaching video on the treatment of news sources. The project was developed to supplement teaching materials for journalism educators.
Trauma and Recovery: The Aftermath of Violence from Domestic Abuse to Political Terror
Integrating clinical and social perspective without sacrificing either the complexity of individual experience or the breadth of political context, "Trauma and Recovery" brings a new level of understanding to the psychological consequences of the full range of traumatic life events.
Achilles in Vietnam: Combat Trauma and the Undoing of Character
Jonathan Shay is a Boston based psychiatrist caring for Vietnam combat veterans diagnosed with severe, chronic post-traumatic stress disorder. In this unique and revolutionary book, Dr. Shay examines the psychological devastation of war by comparing the soldiers of Homer’s Iliad with many of his patients, Vietnam veterans struggling with PTSD . Although the Iliad was written twenty-seven centuries ago, so much can be learned about combat trauma, especially when it is threaded through the compelling voices and experiences of Vietnam vets.
Journalists under Fire: The Psychological Hazards of Covering War
War journalists, like all who have prolonged exposure to violence, come home emotionally maimed and often broken. And yet, a news culture in denial has pretended that war journalists are immune from trauma. This fit into the macho culture of war journalism. It also assuaged the consciences of those running news organizations, who often crumple up and discard, years later, those they send to war. Dr. Feinstein has provided us with research that is a chilling reminder that war journalists are human, as well as a searing indictment of major news conglomerates who have refused to acknowledge or address the suffering of their own.
PTSD and Veterans: A Conversation with Dr. Frank Ochberg
How do we help veterans who are returning from war with PTSD? Dr. Frank Ochberg, a leading authority on PTSD, shares his experiences, seasoned insights and suggestions in this intimate conversation with reporter Mike Walters. He shares his insights regarding common symptoms to look out for and the importance of building trust and other aspects of the patient-therapist relationship. He then explains techniques he has developed that help his clients work through the trauma and adapt to civilian life.
Mapping Trauma and Its Wake: Autobiographic Essays by Pioneer Trauma Scholars
Mapping Trauma and Its Wake is a compilation of autobiographic essays by seventeen of the field's pioneers, each of whom has been recognized for his or her contributions by the International Society for Traumatic Stress Studies. Each author discusses how he or she first got interested in the field, what each feels are his or her greatest achievements, and where the discipline might - and should - go from here. This impressive collection of essays by internationally-renowned specialists is destined to become a classic of traumatology literature. It is a text that will provide future mental health professionals with a window into the early years of this rapidly expanding field.
Post-Traumatic Therapy And Victims Of Violence (Psychosocial Stress Series)
Frank M. Ochberg, MD is adjunct professor of psychiatry, criminal justice and journalism at Michigan State University. He served in the cabinet of Governor William Milliken as Mental Health Director. His book, Post Traumatic Therapy and Victims of Violence, is widely acclaimed as one of the leading resources in the field.
In this long-awaited memoir, Lifton charts the adventurous and surprising course of his fascinating life journey, one that took him from what he refers to as, "a Jewish Huck Finn childhood in Brooklyn, to deep and meaningful friendships with many of the most influential intellectuals, writers, and artists of our time—from Erik Erikson, David Riesman, and Margaret Mead, to Howard Zinn and Kurt Vonnegut, Stanley Kunitz, Kenzaburo Oe, and Norman Mailer.
This work is more than a memoir, it is also a remarkable study of Hiroshima survivors. Lifton explored the human consequences of nuclear weapons, and then went on to uncover dangerous forms of attraction to their power in the spiritual disease he calls nuclearism. Lifton writing illuminates the reversal of healing and killing in ordinary physicians who had been socialized to Nazi evil. Written with the warmth of spirit—along with the humor and sense of absurdity—that have made Lifton a beloved friend and teacher to so many, Witness to an Extreme Century is a moving and deeply thought-provoking story of one man’s extraordinary commitment to looking into the abyss of evil in order to help others move past it.
Odysseus in America: Combat Trauma and the Trials of Homecoming
In this original psychological literary work, Dr. Jonathan Shay continues what he started in his book, Achilles in Vietnam. Uses the Odyssey, the story of a soldier's homecoming, Shay sheds light on the pitfalls that trap many veterans on the road to recovery, the return to civilian life. The combination of psychological insight and literary brilliance feels seamless. Shay makes an impassioned plea to renovate American military institutions and in doing so deepens the readers understanding of the veteran's experience.
Trauma Journalism personalizes this movement with in-depth profiles of reporters, researchers and trauma experts engaged in an international effort to transform how the media work under the most difficult of conditions.Through biographical sketches concerning several significant traumatic events (Oklahoma City bombing, Columbine school tragedy, 9/11, Iraq War, the South Asian tsunami, Hurricane Katrina), students and working reporters will gain insights into the critical components of contemporary journalism practices.
After the War Zone: A Practical Guide for Returning Troops and Their Families
Two experts from the VA National Center for PTSD come together in this work to provide an essential resource for service members, their spouses, families, and communities. They shed light on what troops really experience during deployment and once they return home. Pinpointing the most common after-effects of war and offering strategies for troop reintegration to daily life, Friedman and Slone cover the myths and realities of homecoming; reconnecting with spouse and family; anger and adrenaline; guilt and moral dilemmas; and PTSD and other mental-health concerns. With a wealth of community and government resources, tips, and suggestions, After the War Zone is a practical guide to helping troops and their families prevent war zone stresses from having a lasting negative impact.
Resilience: The Science of Mastering Life's Greatest Challenges
Experiencing trauma at some point in life is almost inevitable, overcoming it is not. This inspiring book identifies ten key ways to weather and bounce back from stress and trauma. Steven M. Southwick incorporates the latest scientific research and interviews with trauma survivors. This book provides a practical guide to building emotional, mental and physical resilience after trauma.
Trauma Therapy in Context: The Science and Craft of Evidence-based Practice
This book examines several current clinical approaches to trauma-focused treatment. Rather than describe theoretical approaches in isolation, the editors have integrated these interventions into a broader clinical context. Chapter authors emphasize basic therapeutic skills such as empathic listening, instilling resilience, and creating meaning, in the service of empirically-supported, highly efficacious trauma interventions. Throughout, they focus on the real-life challenges that arise in typical therapy sessions to deepen our understanding and application of evidence based interventions.
While this book is intended for all clinical mental health professionals who work with trauma survivors it is also a phenomenal resource for those who seek to broaden their understanding of the way various approaches to understanding treatment of trauma.
The award-winning author and noted psychiatrist Robert Jay Lifton offers a powerful critique of American militarism during the Vietnam War. Home from the War is recognized as the ultimate text for those working with Vietnam veterans, the book's insights have had enormous influence among psychologists and psychiatrists all over the world.
The Nazi Doctors: Medical Killing and the Psychology of Genocide
The Boston Globe called this book, "A powerful reminder not only of what happened, but of the monumental evil done by the particular human beings who were trained to heal and cure."
Based on arresting historical scholarship and personal interviews with Nazi and prisoner doctors, the book traces the inexorable logic leading from early Nazi sterilization and euthanasia of its own citizens to mass extermination of "racial undesirables."This extraordinary work combines research and analyzation to describe a seemingly contradictory phenomenon of doctors becoming agents of mass murder. With chilling literary power, Lifton describes the Nazi transmutation of values that allowed medical killing to be seen as a therapeutic healing of the body politic.
When Trauma and Recovery was first published in 1992, it was hailed as a groundbreaking work. In the intervening years, Herman’s volume has changed the way we think about and treat traumatic events and trauma victims. In a new afterword, Herman chronicles the incredible response the book has elicited and explains how the issues surrounding the topic have shifted within the clinical community and the culture at large.
Covering Violence: A Guide to Ethical Reporting About Victims & Trauma
More essential now than ever, Covering Violence connects journalistic practices to the rapidly expanding body of literature on trauma, post-traumatic stress disorder, and secondary traumatic stress, and pays close attention to current medical and political debates concerning victims' rights.
Sharing the Front Line and the Back Hills is a story that points to a crisis facing international institutions and the media who seek to alleviate and report human suffering throughout the world. The goals of the editor are to tell the story of thousands of individuals dedicated to helping others; and to integrate issues of protection and care into all levels of planning, implementing and evaluating international intervention and action. The book identifies approaches that have proven useful and explores and suggests future directions.
The Roots of Evil: The Origins of Genocide and Other Group Violence
Ervin Staub explores the psychological, cultural, and societal roots of group aggression. He sketches a conceptual framework for the many influences on one group's desire to harm another: cultural and social patterns predisposing to violence, historical circumstances resulting in persistent life problems, and needs and modes of adaptation arising from the interaction of these influences.
Drawing on more than 30 years of criminal justice experience, author Susan Herman explains why justice for all requires more than holding offenders accountable it means addressing victims three basic needs: to be safe, to recover from the trauma of the crime, and regain control of their lives.
Arnold Isaacs, who spent the final years of the war in Vietnam as a correspondent for the Baltimore Sun, describes his firsthand observations of the collapse of Cambodia and South Vietnam―from the 1973 Paris peace agreement to the American evacuation of Saigon and its aftermath―with heartbreaking detail, from the devastated battlefields and villages to the boats filled with terrified refugees.
Lost Lives: The Stories of the Men, Women and Children who Died as a Result of the Northern Ireland Troubles
This is the story of the Northern Ireland troubles told as never before. It is not concerned with the political bickering, but with the lives of those who have suffered and the deaths which have resulted from more than three decades of conflict
A Country Called Amreeka: U.S. History Retold through Arab-American Lives
The history of Arab settlement in the United States stretches back nearly as far as the history of America itself. For the first time, Alia Malek brings this history to life. In each of eleven spellbinding chapters, she inhabits the voice and life of one Arab American, at one time-stopping historical moment.
This book seeks to tell the life stories of the innocent men and women who have been needlessly swept up in the “war on terror.” As we approach the ten-year anniversary of 9/11, this collection of narratives gives voice to the people who have had their human rights violated here in the U.S. by post-9/11 policies and actions.
Unsettled/Desasosiego: Children in a World of Gangs/Los niños en un mundo de las pandillas
With profound empathy for a reality that is too easily defined and dismissed as repugnant, Unsettled/Desasosiego takes us on a visual journey into the lives of children deeply affected by civil war and gang violence.
Legal Lynching: The Death Penalty and America's Future
Legal Lynching offers a succinct, accessible introduction to the debate over the death penalty's history and future, exposing a chilling frequency of legal error, systemic racial and economic discrimination, and pervasive government misconduct.
War Photographer is a documentary by Christian Frei about the photographer James Nachtwey. As well as telling the story of an iconic man in the field of war photography, the film addresses the broader scope of ideas common to all those involved in war journalism, as well as the issues that they cover.
Shake Hands with the Devil: The Failure of Humanity in Rwanda
For the first time in the United States comes the tragic and profoundly important story of the legendary Canadian general who "watched as the devil took control of paradise on earth and fed on the blood of the people we were supposed to protect.
Blood and Soil: A World History of Genocide and Extermination from Sparta to Darfur
In Blood and Soil, Kiernan examines outbreaks of mass violence from the classical era to the present, focusing on worldwide colonial exterminations and twentieth-century case studies including the Armenian genocide, the Nazi Holocaust, Stalin’s mass murders, and the Cambodian and Rwandan genocides.
Ophuls examines attitudes toward war in the Western media, and in the societies they inform. The 243-minute documentary interlaces stark realities of combat with mordantly hilarious references to Hollywood fantasy-versions of war, and includes over 50 interviews with some of the world’s leading journalists, commentators, historians, newscasters and many others.
An enthralling, deeply moving memoir from one of our foremost American war correspondents. Janine Di Giovanni has spent most of her career—more than twenty years—in war zones recording events on behalf of the voiceless. From Sarajevo to East Timor, from Sierra Leone to Afghanistan, Iraq, and Somalia, she has been under siege and under fire.
Echoes of Violence: Letters from a War Reporter (Human Rights and Crimes against Humanity)
Echoes of Violence is an award-winning collection of personal letters to friends from a foreign correspondent who is trying to understand what she witnessed during the iconic human disasters of our time--in Iraq, Lebanon, Afghanistan, and New York City on September 11th, among many other places.
It's What I Do: A Photographer's Life of Love and War
War photographer Lynsey Addario’s memoir It’s What I Do is the story of how the relentless pursuit of truth, in virtually every major theater of war in the twenty-first century, has shaped her life.
With inspiring fearlessness, McClelland tackles perhaps her most harrowing assignment to date: investigating the damage in her own mind and repairing her broken psyche. She begins to probe the depths of her illness, exploring our culture's history with PTSD, delving into the latest research by the country's top scientists and therapists, and spending time with veterans and their families.
Annihilating Difference: The Anthropology of Genocide
This ground breaking book, the first collection of original essays on genocide to be published in anthropology, explores a wide range of cases, including Nazi Germany, Cambodia, Guatemala, Rwanda, and Bosnia.
Torture Team: Rumsfeld's Memo and the Betrayal of American Values
In 2002 Donald Rumsfeld signed a memo that authorized the controversial interrogation practices that later migrated to Guantanamo, Afghanistan, Abu Ghraib, and elsewhere. From a behind-the-scenes vantage point, Phillipe Sands investigates how this memo set the stage for divergence.
Shoah is Claude Lanzmann's landmark documentary meditation on the Holocaust. Assembled from footage shot by the filmmaker during the 1970s and 1980s, it investigates the genocide at the level of experience: the geographical layout of the camps and the ghettos; the daily routines of imprisonment; the inexorable trauma of humiliation, punishment, extermination; and the fascinating insights of those who experienced these events first hand.
Humankind has struggled to make sense of human-upon-human violence. Edited by two of anthropology's most passionate voices on this subject, "Violence in War and Peace: An Anthology" is the only book of its kind available: a single volume exploration of social, literary, and philosophical theories of violence.
A gripping and insightful examination of the relationship between news-makers and news-watchers, looking at how images of war and tragedy are presented to us in the media and how we consume them
Guzmán focuses on the similarities between astronomers researching humanity’s past, in an astronomical sense, and the struggle of many Chilean women who still search, after decades, for the remnants of their relatives executed during the dictatorship. Patricio Guzmán narrates the documentary himself and the documentary includes interviews and commentary from those affected and from astronomers and archeologists.
In his extraordinarily gripping and thought-provoking new book, Jeremy Bowen charts his progress from keen young novice whose first reaction to the sound of gunfire was to run towards it to the more circumspect veteran he is today
The Secret Life of War: Journeys Through Modern Conflict
The Observer's chief foreign correspondent Peter Beaumont, takes us into the guts of modern conflict. He visits the bombed and abandoned home of Mullah Omar; discovers a deserted Al Qaeda camp where he finds documents describing a plan to attack London; talks to young bomb-throwers in a Rafah refugee camp. Unflinching and utterly gripping
France's leading sociologist shows how, far from reflecting the tastes of the majority, television, particularly television journalism, imposes ever-lower levels of political and social discourse on us all.
Nickel and Dimed reveals low-rent America in all its tenacity, anxiety, and surprising generosity -- a land of Big Boxes, fast food, and a thousand desperate stratagems for survival. Read it for the smoldering clarity of Ehrenreich's perspective and for a rare view of how "prosperity" looks from the bottom.
Mindfulness: An Eight-Week Plan for Finding Peace in a Frantic World
MINDFULNESS reveals a set of simple yet powerful practices that you can incorporate into daily life to help break the cycle of anxiety, stress, unhappiness, and exhaustion. It promotes the kind of happiness and peace that gets into your bones. It seeps into everything you do and helps you meet the worst that life throws at you with new courage.
Full Catastrophe Living: Using the Wisdom of Your Body and Mind to Face Stress, Pain, and Illness
Full Catastrophe Living is a book for the young and the old, the well, the ill, and anyone trying to live a healthier and saner life in today’s world. By using the practices described within, you can learn to manage chronic pain resulting from illness and/or stress related disorders.
Slee: A Very Short Introduction, addresses the biological and psychological aspects of sleep, providing a basic understanding of what sleep is and how it is measured, a look at sleep through the human lifespan, and the causes and consequences of major sleep disorders.
King Leopold's Ghost: A Story of Greed, Terror, and Heroism in Colonial Africa
King Leopold's Ghost is the haunting account of a megalomaniac of monstrous proportions, a man as cunning, charming, and cruel as any of the great Shakespearean villains. It is also the deeply moving portrait of those who fought Leopold: a brave handful of missionaries, travelers, and young idealists who went to Africa for work or adventure and unexpectedly found themselves witnesses to a holocaust.
This is a new edition of the world's leading textbook on journalism. Translated into more than a dozen languages, David Randall's handbook is an invaluable guide to the 'universals' of good journalistic practice for professional and trainee journalists worldwide.
Legends of People Myths of State: Violence, Intolerance, and Political Culture in Sri Lanka
This provocative study of the political culture of nationalism in Sri Lanka and Australia - is one of the few genuinely comparative studies in anthropology and in taking up such an important question as nationalism it reminds us that truly relevant anthropology questions deep-seated cultural beliefs, including our own
Family Secrets: Shame and Privacy in Modern Britain
Family Secrets offers a sweeping account of how shame--and the relationship between secrecy and openness--has changed over the last two centuries in Britain. Deborah Cohen uses detailed sketches of individual families as the basis for comparing different sorts of social stigma.
During World War Two, 131 German cities and towns were targeted by Allied bombs, a good number almost entirely flattened. Six hundred thousand German civilians died—a figure twice that of all American war casualties. Seven and a half million Germans were left homeless. Given the astonishing scope of the devastation, W. G. Sebald asks: Why?
The Sewing Circles of Herat: A Personal Voyage Through Afghanistan
Christina Lamb's evocative reporting brings to life the stories that no one else had written about: the abandoned victims of almost a quarter century of war. Her unique perspective on Afghanistan and deep passion for the people she writes about make this the definitive account of the tragic plight of a proud nation.
House of Stone: The True Story of a Family Divided in War-Torn Zimbabwe
Christina Lamb's powerful narrative traces the history of the brutal civil war, independence, and the Mugabe years, all through the lives of two people on opposing sides. Although born within a few miles of each other, their experience growing up could not have been more different.
Butcher & Bolt: Two Hundred Years of Foreign Failure in Afghanistan
Butcher & Bolt brilliantly brings to life the personalities involved in Afghanistan’s relationship with the world, chronicling the misunderstandings and missed opportunities that have so often led to war.
Jerusalem 1913: The Origins of the Arab-Israeli Conflict
Jerusalem 1913 shows us a cosmopolitan city whose religious tolerance crumbled before the onset of Z ionism and its corresponding nationalism on both sides-a conflict that could have been resolved were it not for the onset of World War I. With extraordinary skill, Amy Dockser Marcus rewrites the story of one of the world's most indelible divides.
They Fought for Each Other: The Triumph and Tragedy of the Hardest Hit Unit in Iraq
Based on "Blood Brothers," the award-nominated series that ran in Army Times, this is the remarkable story of a courageous military unit that sacrificed their lives to change Adhamiya, Iraq from a lawless town where insurgents roamed freely, to a safe and secure neighborhood. This is a timeless story of men at war and a heartbreaking account of American sacrifice in Iraq.
The War Comes Home: Washington's Battle against America's Veterans
Aaron Glantz reported extensively from Iraq during the first three years of this war and has been reporting on the plight of veterans ever since. The War Comes Home is the first book to systematically document the U.S. government's neglect of soldiers returning from Iraq and Afghanistan.
Madame Dread: A Tale of Love, Vodou, and Civil Strife in Haiti
Kathie Klarreich's compelling memoir interweaves shattering political events with an intensely personal narrative about the Haitian musician Klarreich, who turns out to be as enthralling and complicated as the political events she covered.
In the tradition of Helter Skelter and In Cold Blood, Columbine is destined to be a classic. A close-up portrait of hatred, a community rendered helpless, and the police blunders and cover-ups, it is a compelling and utterly human portrait of two killers-an unforgettable cautionary tale for our times
Juvenile, photographer Joseph Rodríguez spent several years following several youths, from arrest, counseling, trial adjudication, and incarceration, to release, probation, house arrest, group homes, and the search for employment and meaning in their lives.
By age twelve, Luis Rodriguez was a veteran of East Los Angeles gang warfare. This story is at times heartbreakingly sad and brutal, Always Running is ultimately an uplifting true story, filled with hope, insight, and a hard-earned lesson for the next generation.
Still Here, documents the ongoing expressions of hope, perseverance, and suffering in the still-devastated communities of New Orleans and Texas post hurricane Katrina. Rodríguez spent two years photographing and interviewing families and individuals who shared their daily struggles to rebuild their lives.
Breaking News, Breaking Down, Two journalists' emotional journey after 9/11 & Katrina - This program tells the hidden story of how traumatic news impacts the men and women who cover it. Mike Walter loved chasing the big story, but on one September morning, the biggest story of his career chased him down: a jet rained from the sky, piercing the Pentagon and shattering his emotional well being.
One of the Guys: Women as Aggressors and Torturers
The debate about women and torture has, until recently, focused on women as victims of violence. The essays in One of the Guys challenge and examine the expectations placed on women while attempting to understand female perpetrators of abuse and torture in a broader context.
Monstering: Inside America's Policy of Secret Interrogations and Torture in the Terror War
Tara McKelvey — the first U.S.journalist to speak with female prisoners from Abu Ghraib — traveled to the Middle East and across the United States to seek out victims and perpetrators. McKelvey tells how soldiers, acting in an atmosphere that encouraged abuse and sadism, were unleashed on a prison population of which the vast majority, according to army documents, were innocent civilians.
Gogo Mama : A Journey Into the Lives of Twelve African Women
This book is a journey across Africa, in all its complexity; from the townships of Johannesburg, to the back alleys of Zanzibar; from the frontline of the war in the Sudan, to the nightclubs of Cairo. It is a vivid, illuminating and often haunting composite picture of an extraordinary continent, in the words of the women who know it best.
Shaking the Foundations: 200 Years of Investigative Journalism in America
This is the first anthology of its kind, bringing together outstanding practitioners of the muckraking tradition, from the Revolutionary era to the present day. Ranging from mainstream figures like Woodward and Bernstein to legendary iconoclasts such as I. F. Stone and Ida B. Wells-Barnett, the dispatches in this collection combine the thrill of the chase after facts with a burning sense of outrage
Trauma Therapy in Context: The Science and Craft of Evidence-based Practice
This book examines several current clinical approaches to trauma-focused treatment. Rather than describe theoretical approaches in isolation, the editors have integrated these interventions into a broader clinical context. Chapter authors emphasize basic therapeutic skills such as empathic listening, instilling resilience, and creating meaning, in the service of empirically-supported, highly efficacious trauma interventions.
Ari Goldman’s exploration of the emotional and spiritual aspects of spending a year in mourning for his father will resonate with anyone who has lost a loved one, as he describes how this year affected him as a son, husband, father, and member of his community.
What began as a project to deepen his knowledge of the world’s sacred beliefs turned out to be an extraordinary journey of spiritual illumination, one in which Goldman reexamined his own faith as an Orthodox Jew and opened his mind to the great religions of the world. Written with warmth, humor, and penetrating clarity, The Search for God at Harvard is a book for anyone who has wrestled with the question of what it means to take religion seriously today.
Being Jewish: The Spiritual and Cultural Practice of Judaism Today
In Being Jewish, Ari L. Goldman offers eloquent thoughts about an absorbing exploration of modern Judaism. A bestselling author and widely respected chronicler of Jewish life, Goldman vividly contrasts the historical meaning of Judaism's heritage with the astonishing and multiform character of the religion today.
This book is a collection of reflective crime pieces, often approaching the events from different angles, yet written by on-the spot observers and reporters. There is an emphasis on the victims, and as a result these stories are written with sensitivity and compassion rather than sensationalism.
Over twenty-five tales of grisly murders and suspicious killings are laid out for inspection, including the story of the Police Killers and tales of the seedy Melbourne underworld.
This fully revised and updated new edition of Smart Health Choices will provide you with the tools for assessing health advice, whether it comes from a specialist, general practitioner, naturopath, the media, the Internet, or a friend. It shows you how to take an active role in your health care, and to make the best decisions for you and your loved ones based on personal preferences and the best available evidence.
The Spanish-language version of the Dart Center's 40-page guide to help journalists, photojournalists and editors report on violence while protecting both victims and themselves.
9/11: Mental Health in the Wake of Terrorist Attacks
This book comprehensively describes the psychological response to the 9/11 terrorist attacks in New York and, to a lesser degree, Washington DC. The impact of what happened on the local and US national population is considered through various epidemiological studies, as well as personal accounts from some of those more directly involved.
Filled with astonishing personal stories, conflict, and drama, Feet to the Fire gives readers the rare opportunity to walk a mile in the shoes of this nation’s most powerful journalists and news executives and experience their highly stressful environments. With each new and revealing interview, Borjesson gathers devastating details from national security and intelligence reporters, White House journalists, Middle East experts, war correspondents, and others. Like pieces of a terrible puzzle, these conversations combine to provide a hair-raising view of the mechanisms by which the truth has been manufactured post 9/11.
Chronicling Trauma: Journalists and Writers on Violence and Loss
Grounded in the latest research in the fields of trauma studies, literary biography, and the history of journalism, this study draws upon the lively and sometimes breathtaking accounts of popular writers such as Charles Dickens, Ernest Hemingway, Dorothy Parker, Graham Greene, and Truman Capote, exploring the role that trauma has played in shaping their literary works. Underwood notes that the influence of traumatic experience upon journalistic literature is being reshaped by a number of factors, including news media trends, the advance of the Internet, the changing nature of the journalism profession, the proliferation of psychoactive drugs, and journalists' greater self-awareness of the impact of trauma in their work.
Daring to Feel: Violence, the News Media, and Their Emotions
Daring to Feel is a bold, brave book. Jody Santos challenges the entrenched doctrine that journalists are neutral, dispassionate observers of 'fact.' Santos demonstrates how journalists themselves and society as a whole benefit from emotionally nuanced and emotionally engaged reporting. This is a beautifully written tribute to the passion of journalists and the heart-wrenching stories they cover.
The Things They Cannot Say: Stories Soldiers Won't Tell You About What They've Seen, Done or Failed to Do in War
In The Things They Cannot Say, award-winning journalist and author Kevin Sites asks these difficult questions of eleven soldiers and marines, who—by sharing the truth about their wars—display a rare courage that transcends battlefield heroics. For each of these men, many of whom Sites first met while in Afghanistan and Iraq, the truth means something different. One struggles to recover from a head injury he believes has stolen his ability to love; another attempts to make amends for the killing of an innocent man; yet another finds respect for the enemy fighter who tried to kill him. Sites also shares the unsettling narrative of his own failures during war—including his complicity in a murder—and the redemptive powers of storytelling that saved him from a self-destructive downward spiral.
Kevin Sites, the award-winning journalist, covered virtually every major global hot spot as the first Internet correspondent for Yahoo! News. Beginning his journey with the anarchic chaos of Somalia in September 2005 and ending with the Israeli-Hezbollah war in the summer of 2006, Sites talks with rebels and government troops, child soldiers and child brides, and features the people on every side, including those caught in the cross fire. His honest reporting helps destroy the myths of war by putting a human face on war's inhumanity.
Swimming with Warlords: A Dozen-Year Journey Across the Afghan War
Using his trademark immersive style, Kevin Sites uncovered surprising stories with unexpected truths. He swam in the Kunduz River with an infamous warlord named Nabi Gechi, who demonstrated both his fearsome killing skills as well as a genius for peaceful invention. Sites talked with ex-Taliban fighters, politicians, female cops, farmers, drug addicts, and diplomats, and patrolled with American and Afghan soldiers. In Swimming with Warlords he helps us to understand this kingdom of primitive beauty, dark mysteries, and savage violence, as well as the conflict that has cost billions of dollars and thousands of lives--and what we might expect tomorrow and in the years to come.
The Price They Paid is the stunning and dramatic true story of a legendary helicopter commander in Vietnam and the flight crews that followed him into the most intensive helicopter warfare ever—and how that brutal experience has changed their lives in the forty years since the war ended.
What Have We Done: The Moral Injury of Our Longest Wars
Most Americans are now familiar with PTSD and its prevalence among troops. In this groundbreaking book, David Wood examines the far more pervasive yet less understood experience of those we send to war: moral injury, the violation of our fundamental values of right and wrong that so often occurs in the impossible moral dilemmas of modern conflict.
Collective Conviction: The Story of Disaster Action
Collective Conviction tells the story of Disaster Action, a small charity founded in 1991 by survivors and bereaved people from the disasters of the late 1980s, including Zeebrugge, King's Cross, Clapham, Lockerbie, Hillsborough and the Marchioness. The aims were to create a health and safety culture in which disasters were less likely to occur and to support others affected by similar events.
When Lynne O’Donnell met Pauline and Margaret in Iraq she could never have guessed the wealth of stories she’d discover. Over tea the two women tell Lynne of their lives in the country: each having married Iraqi men had then relocated from England more than thirty years before.
Trauma Reporting A Journalist's Guide to Covering Sensitive Stories
Trauma Reporting provides vital information on developing a healthy, professional and respectful relationship with those who choose to tell their stories during times of trauma, distress or grief.